

Executive Summary
Solid-tumor CAR-T reached a genuine inflection point in 2026. The first approval establishes that an autologous CAR-T product can produce enough controlled clinical benefit in an epithelial cancer to support marketing authorization. The magnitude of that benefit, however, is materially smaller than the transformative responses that defined CAR-T in B-cell malignancies.
The strongest remaining programs divide into distinct evidence tiers. Some adult epithelial-tumor assets have generated response rates that are difficult to dismiss, but the datasets remain small, nonrandomized, and vulnerable to selection effects. Pediatric neuroblastoma and diffuse midline glioma programs show deeper and sometimes durable individual responses, although their biology, delivery methods, and patient selection limit extrapolation to common adult solid tumors.
The central diligence question is no longer whether a solid-tumor CAR-T can cause tumor regression. Several can. The harder question is whether an asset can produce durable benefit across an intent-to-treat population after manufacturing time, pre-infusion progression, antigen heterogeneity, on-target toxicity, lymphodepletion, repeated dosing, and specialized hospital care are included.
CAR-T in Brief: From Blood Cancers to Solid Tumors
CAR-T (chimeric antigen receptor T-cell) therapy is a form of adoptive cellular immunotherapy in which a patient's T cells are collected, genetically engineered to express a chimeric antigen receptor, expanded outside the body, and infused back into the patient. The engineered receptor combines an antigen-binding component with intracellular signaling domains, allowing the modified T cells to recognize a selected surface antigen and activate an antitumor response. 1
The established clinical model is hematologic, or non-solid, cancer. In the United States, U.S. Food and Drug Administration (FDA)-approved CAR-T products are used for B-cell leukemias and lymphomas or multiple myeloma. These therapies can produce deep and sometimes durable remissions in heavily pretreated patients, although relapse and serious treatment-related toxicities remain important limitations. 12
Solid tumors present additional biological and operational barriers. Target antigens may also be expressed on normal tissue, antigen expression can vary within and between tumors, and the tumor microenvironment can limit T-cell trafficking, persistence, and function. Solid-tumor programs therefore need to demonstrate more than initial shrinkage: selectivity, durability, deliverability, and effectiveness across the full intended population are central to the development case. 1
The 2026 Inflection Point: Satri-cel
On June 22, 2026, China's National Medical Products Administration approved satricabtagene autoleucel, or satri-cel, for claudin-18 isoform 2 (CLDN18.2)-positive, human epidermal growth factor receptor 2 (HER2)-negative advanced gastric or gastroesophageal junction adenocarcinoma after failure of at least two prior lines of therapy. The approval made satri-cel the first marketed CAR-T product for a solid tumor. The geographic scope matters: this is a Chinese approval in a biomarker-selected gastric-cancer population, not yet a broad global validation of the class. 3
The underlying randomized phase 2 study enrolled 156 patients at 24 hospitals in China and assigned them 2:1 to satri-cel or physician's choice. Median progression-free survival (PFS) was 3.25 months versus 1.77 months, an absolute gain of 1.48 months. Median overall survival (OS) was 7.92 months versus 5.49 months, an absolute gain of 2.43 months. The confirmed objective response rate (ORR) was 22% with satri-cel and 4% with physician's choice, while median response duration with satri-cel was 5.52 months. 4
The result is clinically meaningful because it is randomized, biomarker-defined, and positive in a heavily pretreated population. It is also important not to overstate it. The overall-survival hazard ratio was 0.69 with a 95% confidence interval of 0.46 to 1.05, so the point estimate favors satri-cel but remains imprecise. The treatment effect is therefore best understood as the first controlled proof that CAR-T can improve outcomes in a common epithelial cancer, not evidence that solid-tumor CAR-T has reproduced the magnitude or durability seen in the most responsive hematologic settings. 4
Operational attrition was visible even in the successful program. Sixteen patients assigned to satri-cel were not infused because their disease progressed during the treatment interval. Grade 3 or higher adverse events occurred in 99% of satri-cel recipients, cytokine release syndrome occurred in 95%, and one treatment-related death occurred in each trial group. These findings mean that manufacturing speed and patient selection are part of the treatment effect, not secondary implementation details. 4
Evidence Map
Reported antitumor activity against the maturity of the supporting clinical evidence is mapped below. The vertical axis shows the reported percentage of evaluable patients with objective activity, while the horizontal axis progresses from company-reported findings through replicated signals, mature single-arm datasets, and randomized evidence. Bubble area reflects the approximate efficacy-analysis population, and color distinguishes adult epithelial, central nervous system (CNS), and pediatric programs. The figure should not be read as a direct cross-trial efficacy comparison: tumor type, antigen threshold, prior therapy, response criteria, dose, route of administration, follow-up, and evaluable-population definitions differ across programs.
Solid-Tumor CAR-T: Activity vs Evidence Strength
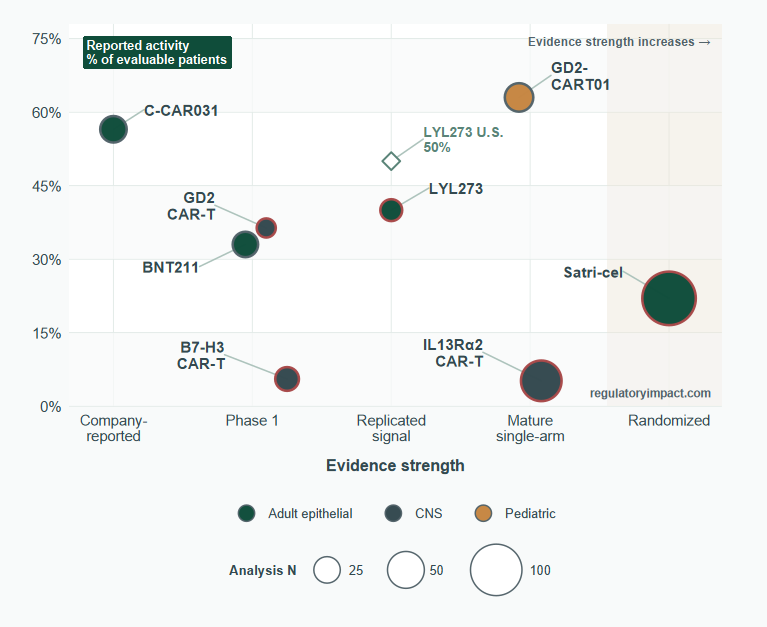
The central pattern is a separation between headline activity and evidentiary confidence. C-CAR031 and GD2-CART01 occupy the high-activity region, but their estimates remain based on relatively small, nonrandomized datasets. LYL273 has a lower reported response rate than those programs, yet activity has appeared in separate Chinese and U.S. cohorts, moving the program further to the right because the signal has been replicated. Satri-cel sits lower on the activity axis, at a 22% confirmed objective response rate, but furthest to the right because it is supported by randomized evidence. Its position illustrates the main interpretive point: a smaller effect measured with a stronger design can be more developmentally consequential than a larger effect observed in a small early-phase cohort. 45678
The CNS programs also require a different reading. Their lower placement on a response-rate axis does not fully capture exceptional durable responses, prolonged disease stabilization, local delivery, repeat dosing, or survival hypotheses derived from historical comparisons. The table below therefore supplies the context that the figure intentionally compresses, including durability, denominator, study design, and the principal limitations of each dataset. It is a hierarchy of evidence, not a league table. 91011
The development picture below prioritizes programs with interpretable human efficacy data; it does not rank assets supported only by preclinical findings or sparse disclosures. Cross-trial response rates are not directly comparable because tumor types, antigen thresholds, prior therapy, response criteria, dose, route of administration, and evaluable-population definitions differ. The table is therefore a hierarchy of evidence, not a league table. 45671213891011
| Asset | Target and setting | Most informative efficacy signal | Evidence-quality assessment |
|---|---|---|---|
| Satri-cel | CLDN18.2; third-line or later gastric or gastroesophageal junction adenocarcinoma | Randomized phase 2: ORR 22% vs 4%; median PFS 3.25 vs 1.77 months; median OS 7.92 vs 5.49 months | Highest-confidence solid-tumor CAR-T dataset. Benefit is real but modest in absolute duration. |
| LYL273, formerly GCC19CART | Guanylyl cyclase C (GCC); refractory metastatic colorectal cancer | China phase 1: ORR 40% in 15 patients and median OS 22.8 months. U.S. company update: ORR 50% in 12 patients and 67% in 6 patients at the higher dose | Reproducible activity across two small cohorts, but no randomized benchmark and material gastrointestinal toxicity. |
| C-CAR031, also called AZD7003 | Glypican 3 (GPC3); advanced hepatocellular carcinoma | Company-reported phase 1: ORR 56.5% and disease control rate (DCR) 91.3% among 23 evaluable patients; estimated median OS 11.14 months | Large raw response signal for an adult epithelial tumor, but single-arm, early, and without mature response-duration data in the disclosed summary. |
| BNT211 | Claudin-6 (CLDN6); mixed relapsed or refractory solid tumors | Peer-reviewed phase 1: unconfirmed ORR 33% in 21 evaluable patients; median response duration 2.8 months; ORR 57% in a 7-patient high-dose germ-cell-tumor subgroup | Demonstrates biological activity, but pooled durability was short and the dedicated phase 2 germ-cell-tumor study is listed as terminated or withdrawn. |
| GD2-CART01 | GD2 (a disialoganglioside); relapsed or refractory high-risk neuroblastoma | ORR 63% in 27 patients; among 21 at the recommended dose, 3-year OS 60% and event-free survival 36% | One of the strongest durable single-arm signals, but in a pediatric neural-crest tumor with limited generalizability to adult epithelial cancers. |
| GD2-CAR T | GD2; histone H3 lysine 27-to-methionine mutation (H3K27M)-positive diffuse midline glioma | Four major volumetric reductions among 11 treated patients, including one complete response ongoing beyond 30 months | Convincing activity in individual patients, with intensive neurotoxicity management and no controlled survival estimate. |
| B7-H3 CAR T | B7 homolog 3 (B7-H3); diffuse intrinsic pontine glioma | One partial response among 18 imaging-evaluable patients; 15 had stable disease; median survival from diagnosis was 19.8 months in 21 treated patients | A survival hypothesis rather than a strong radiographic-response dataset. Historical comparisons are vulnerable to selection and timing bias. |
| IL13Ralpha2 CAR T | Interleukin-13 receptor alpha 2 (IL13Ralpha2); recurrent high-grade glioma | Two partial responses and one complete response among 58 response-evaluable patients; recurrent glioblastoma median OS 7.7 months | Large phase 1 experience confirms feasibility, but average antitumor activity was modest and most benefit was disease stabilization rather than objective response. |
Adult Epithelial Tumors: Signals Worth Taking Seriously
LYL273 has one of the more credible response signals after satri-cel because activity has appeared in separate Chinese and U.S. cohorts. In the peer-reviewed Chinese phase 1 trial, 6 of 15 patients with metastatic colorectal cancer had partial responses, producing a 40% ORR. Median overall survival was 22.8 months, and median progression-free survival was 6.0 months in the seven-patient higher-dose cohort. Those survival results are notable, but they remain uncontrolled and can be materially influenced by eligibility, disease biology, subsequent therapy, and the small denominator. 5
The U.S. dataset was stronger numerically but less mature and company-reported. Across 12 patients at two dose levels, the ORR was 50%; at the higher dose, 4 of 6 patients responded for a 67% ORR, with median progression-free survival of 7.8 months. The small denominator is critical. One additional response or nonresponse would move a six-patient response rate by almost 17 percentage points. The appropriate interpretation is a clear proof-of-activity signal that merits expansion, not a stable estimate of commercial efficacy. 6
LYL273 also illustrates why a target-specific toxicity can define the product profile. In the Chinese study, 14 of 15 patients developed diarrhea and eight had grade 3 diarrhea. In the first U.S. disclosure, one higher-dose patient had a dose-limiting toxicity that included grade 4 enterocolitis and later died from fungal sepsis. By May 2026, Lyell reported that gastrointestinal prophylaxis reduced grade 2 or higher diarrhea or colitis from 55% in nine patients without prophylaxis to 10% in ten patients with prophylaxis. The amended trial can expand into a potential single-arm phase 2 study pending regulatory alignment, but no new efficacy analysis accompanied the June 2026 safety update. 5614
C-CAR031 has produced a large disclosed response rate in an adult epithelial-tumor program. In an investigator-initiated phase 1 study in advanced hepatocellular carcinoma, 23 of 24 treated patients were efficacy-evaluable. AbelZeta reported an ORR of 56.5%, a disease control rate of 91.3%, and an ORR of 75% at the fourth dose level. At 9.03 months of median follow-up, estimated median overall survival was 11.14 months. Cytokine release syndrome occurred in 91.7%, mostly grade 1 or 2, with one grade 3 event and no reported dose-limiting toxicity. 7
The C-CAR031 result is difficult to dismiss as random noise, but the available disclosure does not establish mature duration of response, comparative survival benefit, or reproducibility outside the initial Chinese study. A response rate above 50% in advanced hepatocellular carcinoma would be highly consequential if it persists in a larger, prospectively defined population. Until that occurs, the asset should be classified as a high-potential phase 1 signal rather than a de-risked late-stage program. 7
BNT211 offers a useful counterexample to reading an early response rate in isolation. The peer-reviewed phase 1 basket study reported an unconfirmed ORR of 33% in 21 evaluable patients, including one complete response, and an ORR of 57% in seven high-dose germ-cell-tumor patients. However, median duration of response across responders was only 2.8 months, and two of the initial partial responses had progressive disease at the next assessment. BioNTech's dedicated phase 2 BNT211-02 germ-cell-tumor study is now listed as terminated or withdrawn, with no reason specified on the trial page. That status does not prove the platform lacks activity, but it weakens the development case for the specific phase 2 path that had been planned. 1213
Pediatric and CNS Programs: Deeper Responses, Harder Interpretation
GD2-CART01 in relapsed or refractory high-risk neuroblastoma remains one of the strongest demonstrations that CAR-T can produce durable benefit in a solid tumor. Seventeen of 27 patients responded, including nine complete responses. Among 21 patients treated at the recommended dose, 3-year overall survival was 60% and 3-year event-free survival was 36%. The absence of a randomized comparator prevents a precise causal survival estimate, and outcomes were substantially better in patients with lower disease burden, but the depth and persistence of response are more compelling than a transient phase 1 shrinkage signal. 8
In H3K27M-positive diffuse midline glioma, sequential intravenous and intracerebroventricular GD2-CAR T treatment produced major volumetric tumor reductions of 52%, 54%, 91%, and 100% in four of 11 treated patients, with three additional smaller reductions. One complete response remained ongoing beyond 30 months. These are genuine antitumor effects in a disease where regression is unusual, but the study was highly selected and explicitly could not support a valid historical survival comparison. 9
The therapeutic burden in the GD2 diffuse-midline-glioma study was substantial. Three patients at the higher intravenous dose had dose-limiting grade 4 cytokine release syndrome, establishing the lower dose as the maximum tolerated intravenous dose. Nine patients then received intracerebroventricular dosing without a dose-limiting toxicity, but every treated patient developed tumor inflammation-associated neurotoxicity that required intensive monitoring and management. The result supports continued development, but it is not a simple one-time outpatient cell infusion. 9
B7-H3 CAR-T in diffuse intrinsic pontine glioma (DIPG) generated a different efficacy pattern. Among 18 imaging-evaluable patients, one had a partial response, 15 had stable disease, and two had progressive disease. Among 21 treated patients, median survival from the first infusion was 10.7 months and median survival from diagnosis was 19.8 months; three patients were alive more than 44 months after diagnosis. The investigators themselves identified immortal-time and historical-control limitations, changes in supportive care, post-protocol therapies, and favorable tumor biology in some long survivors. The data justify a phase 2 test, but they do not yet prove a survival benefit. 10
The larger IL13Ralpha2 glioma experience shows how exceptional responders can coexist with modest average efficacy. Of 92 enrolled patients, CAR-T products were manufactured for 89, but 24 progressed too rapidly to receive the product. Sixty-five patients were infused and 58 were response-evaluable. Two had partial responses and one had a complete response on protocol; 29 patients had stable disease or better, but only 13 maintained confirmed stable disease or better for at least 90 days. Median overall survival was 7.7 months in recurrent glioblastoma. A post hoc arm with optimized manufacturing and dual delivery had median survival of 10.2 months, but the comparison was nonrandomized and potentially confounded. 11
Safety, Delivery, and Attrition Are Part of the Effect Size
Solid-tumor CAR-T efficacy is commonly reported among infused or response-evaluable patients, while the clinically relevant denominator begins earlier. Satri-cel lost 16 assigned patients before infusion because of rapid progression. The IL13Ralpha2 glioma trial successfully manufactured product for 89 patients but infused only 65, largely because 24 patients progressed during the interval. In diseases measured in weeks or a few months, vein-to-vein time can erase a substantial fraction of nominal response benefit. 411
On-target, off-tumor toxicity can also narrow the usable dose. GCC targeting produced diarrhea in 93% of the Chinese GCC19CART cohort and required corticosteroids, dasatinib, or infliximab for severe cases. The U.S. LYL273 program added a multi-agent prophylaxis strategy that included infliximab, vedolizumab, and budesonide. Reducing gastrointestinal toxicity is a meaningful development advance, but prophylactic immunosuppression, infection risk, and treatment complexity must be evaluated alongside response rate. 5614
For CNS tumors, local delivery may improve exposure while creating a specialized treatment model. The B7-H3 DIPG trial administered 253 intracerebroventricular doses to 21 patients, including multiyear repeat dosing in some long survivors. The GD2 diffuse-midline-glioma study combined intravenous priming with repeated intracerebroventricular infusions and intensive neurocritical monitoring. These approaches can be clinically justified in lethal rare diseases, but they make scalability, center qualification, catheter management, and attribution of benefit materially different from a conventional single-infusion CAR-T model. 109
How to Read the Next Wave of Data
First, use the earliest clinically relevant denominator. A response rate among infused patients can be accurate yet overstate practical effectiveness if a meaningful fraction of enrolled or assigned patients deteriorate before manufacturing is complete. Trials should disclose screened, leukapheresed, successfully manufactured, lymphodepleted, infused, and response-evaluable populations separately. 411
Second, separate confirmed response from first-scan shrinkage. BNT211 reported an unconfirmed 33% ORR, and two initial partial responses were followed by progression at the next assessment. Small early trials should show confirmation rate, waterfall plots, time to response, duration of response, and progression pattern rather than relying on a headline ORR. 12
Third, treat dose-level response rates as exploratory until replicated. LYL273's 67% ORR was four responses among six higher-dose patients, while C-CAR031's 75% ORR at dose level 4 came from an early dose-escalation cohort. These results can guide dose selection, but they are too sensitive to single-patient outcomes to define the expected treatment effect. 67
Fourth, distinguish objective regression from prolonged stabilization and from survival comparisons against historical controls. The B7-H3 DIPG study had only one partial response among 18 imaging-evaluable patients despite a potentially favorable survival pattern. The IL13Ralpha2 glioma study reported stable disease or better in half of response-evaluable patients, but only three protocol-defined objective responses. Both programs may have activity, but neither supports a conventional high-ORR narrative. 1011
Finally, require a product-level explanation for durability. Antigen density and homogeneity, trafficking, local delivery, cell expansion, repeat dosing, armoring, lymphodepletion, and rescue immunosuppression are not interchangeable engineering details. Satri-cel now provides the minimum controlled benchmark: a program should eventually show that its technical strategy improves a clinically meaningful endpoint, not merely that engineered cells can enter a tumor and cause temporary shrinkage. 41259
Regulatory and Development Implications
Satri-cel changes the regulatory discussion because the class now has an approved solid-tumor precedent in China, supported by randomized evidence. The precedent is narrower than the phrase 'first solid-tumor CAR-T approval' may imply. It concerns a defined antigen threshold, a specific gastrointestinal malignancy, a late-line population, a proprietary preconditioning regimen, and a Chinese development and regulatory context. Sponsors should not assume that a small single-arm ORR dataset in another tumor type will receive the same evidentiary treatment. 34
LYL273 is the clearest near-term test of whether a high early response rate can support an accelerated single-arm development path in a common adult solid tumor. The U.S. study has been amended to permit a potential pivotal phase 2 expansion, but Lyell states that this depends on regulatory alignment and that the maximum tolerated dose has not yet been determined. The next efficacy update must show whether responses persist after the prophylaxis change and as the denominator expands beyond the original 12 patients. 614
C-CAR031 requires the same transition from signal generation to estimate stabilization. The phase 1 response rate is high enough to justify substantial interest, but the next meaningful dataset should provide confirmed response, median duration of response, progression-free survival, treatment attrition, antigen-expression rules, and outcomes across prospectively selected dose and manufacturing conditions. Without those elements, the 56.5% ORR remains an encouraging but incomplete measure of treatment effect. 7
BNT211 demonstrates that a technically sophisticated platform and a responsive subgroup do not guarantee a clean phase 2 path. The phase 1 study showed CAR-T expansion, responses, and manageable early cytokine-release toxicity, but pooled response duration was short and the dedicated germ-cell-tumor phase 2 study is listed as terminated or withdrawn. Development status should therefore be verified at the trial and indication level rather than inferred from continued appearance of an asset in broad platform descriptions. 1213
Conclusion
Solid-tumor CAR-T is clinically real in 2026, but it is not yet a uniformly validated therapeutic class. Satri-cel provides the decisive proof that a CAR-T product can improve randomized outcomes and receive approval in an epithelial cancer. It also sets a sobering benchmark: the first success delivered a modest absolute survival gain, substantial toxicity, and visible pre-infusion attrition.
The most credible next assets are those that combine repeated evidence of tumor regression with an operationally manageable product profile. LYL273 and C-CAR031 have response signals large enough to warrant serious attention, but both still need larger, more stable estimates of durability and net clinical benefit. BNT211 shows why early activity can fail to translate into a straightforward phase 2 program.
Pediatric neuroblastoma and CNS programs provide some of the deepest individual responses in the field, including durable complete responses. Their results are scientifically important and potentially clinically meaningful, but they often rely on highly selected populations, specialized local delivery, repeated dosing, and historical comparisons. The field's next phase will be determined less by isolated response headlines and more by controlled benefit, durability, manufacturability, treatment access, and the proportion of intended patients who actually receive an effective dose.